
What Will It Take for a New Standard of Care in Cognitive Decline?
Take a moment to imagine precision medicine for Alzheimer's being recommended with as much force and speed as the current cancer standard of care.

This week I came across an article about Lequembi, a treatment for Alzheimer’s disease. It is a new formulation of Lecanemab and what stood out was how simple it has become to administer.
Patients can now inject it themselves at home. It represents the culmination of decades of pharmaceutical development: a drug that’s easier than ever to deliver, more accessible than ever, and yet still fundamentally limited in what it can achieve.
Like other monoclonal antibodies, Lecanemab is designed to clear amyloid plaques from the brain. That’s been the central dogma of Alzheimer’s drug development for years. And while these drugs have shown some ability to slow the rate of decline, they do not restore lost function.
The most striking evidence of this came from a 2022 paper in the Journal of Alzheimer’s Disease. The paper compared outcomes across different approaches: no treatment, taking available medications, and engaging in precision medicine. The graph tells the story in a glance: doing nothing leads to rapid decline; medications slow the slide somewhat; but none of them stop, let alone reverse, the disease.
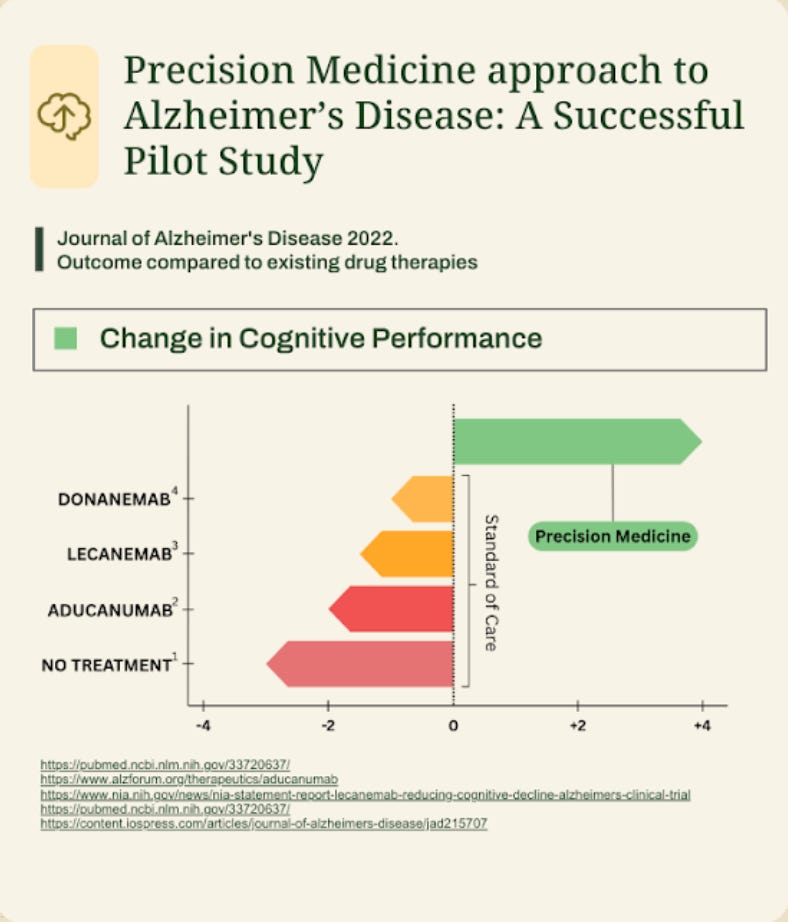
This is where precision medicine enters the conversation. For the first time, we may be on the edge of something that can actually halt or reverse the process of cognitive decline.
Why Precision Medicine Represents a Breakthrough
Precision medicine is fundamentally different from drug-based standards of care because it takes into account the complexity of the human body. Instead of searching for a single “magic bullet,” it looks at a wide range of factors that contribute to brain health.
That includes:
Metabolic health (insulin resistance, blood sugar regulation, nutrient status)
Cardiovascular health (blood pressure, vascular integrity, lipid markers)
Hormonal balance (thyroid, sex hormones, cortisol rhythms)
Toxic exposures (heavy metals, mold and biotoxins, environmental chemicals)
Lifestyle factors (sleep, exercise, stress resilience, social connection)
When we take all of these factors into account and systematically address them, the brain can often recover function—even in cases where decline seemed inevitable.
So what will it take for a new standard of care to emerge?
Step 1: Replicable Clinical Outcomes
The first requirement for any new standard of care is evidence. The precision medicine approach to Alzheimer’s was brought into mainstream conversation by Dr. Dale Bredesen and colleagues, who published case studies and clinical data showing that patients could actually regain cognitive function.
Skeptics have pointed out that these early studies were not placebo-controlled. That’s why the ongoing randomized controlled trial is so important. This trial is designed to demonstrate that precision medicine doesn’t just produce anecdotal improvements, but reliably outperforms placebo across a population.
Early conference presentations suggest highly promising results, with a preprint expected this December and full publication in spring. If the published outcomes confirm what’s been seen in earlier cohorts, we’ll be standing at the threshold of a paradigm shift: the first therapy to not just slow, but reverse cognitive decline.
Step 2: Integrated Diagnostics
Right now, implementing precision medicine for cognitive decline is cumbersome. A clinician has to order labs from multiple companies to get a complete picture: one panel for toxins, another for inflammatory markers, another for cardiovascular health, and so on.
This patchwork approach is time-consuming, confusing for patients, and hard for doctors to organize and interpret at scale. It’s not the kind of system that can become a standard of care.
For precision medicine to scale, we need:
A unified lab ordering system – one portal where clinicians can request all the relevant tests.
Standardized reporting – so results come back in a format that is easy to compare and track.
Clinical decision support – AI-powered tools that help doctors see patterns and generate care plans based on the data.
That’s exactly the infrastructure we’re building at TruNeura: a system that makes it easy to order, track, and interpret the labs required for cognitive restoration.
Step 3: Organized Care Delivery
Even with solid evidence and better tools, a new standard of care doesn’t happen automatically. It requires a pathway that doctors and patients alike can trust.
Oncology provides a useful parallel. If you are diagnosed with a certain type of cancer, there is a clear standard of care: chemotherapy, radiation, or surgery, depending on the case. Patients are quickly funneled into this pathway.
Imagine a future where the same is true for cognitive decline. The moment a patient is diagnosed with mild cognitive impairment or early dementia, they are strongly encouraged, if not effectively required, to begin a precision medicine program. The system makes it easy: every clinic has access to the same streamlined protocols, and insurance recognizes and reimburses the process.
This is what it means for precision medicine to move from being an alternative to being the standard of care.
The Insurance Barrier
Of course, cost is the biggest obstacle. Right now, patients often have to pay out-of-pocket for functional and precision medicine programs. That creates a perception of high expense.
But in healthcare, cost is mostly about coverage. Consider how every drug commercial ends: “See how you can get started for as little as $0.” The actual list price of these drugs is enormous, but insurance coverage and manufacturer assistance programs make them accessible to patients.
Until insurance companies recognize precision medicine as a reimbursable intervention, it will remain in the “expensive” category. The tipping point will come when payers realize that reversing cognitive decline is not just better for patients, but more cost-effective for the system than managing decades of decline and memory care.
What This Future Could Look Like
Here’s the vision:
Early detection becomes standard. Routine cognitive screening identifies subtle decline sooner.
Precision programs are activated immediately. Instead of being told to “wait and see,” patients are given a pathway that integrates labs, lifestyle, and targeted therapies.
Clinicians are empowered. Every doctor has the tools to deliver precision brain health without needing to reinvent the wheel.
Insurance shifts. Once reversal is proven, payers recognize the long-term savings and make precision medicine accessible at scale.
In this future, losing your memory is no longer an inevitable part of aging. Instead, early intervention restores function and helps people live longer, sharper lives.
The Role of TruNeura
At TruNeura, our mission is to accelerate this transition. We’re building the infrastructure that makes precision medicine for cognitive decline practical: integrated lab systems, clinician dashboards, and patient engagement tools.
While consumer apps and wearables have their place, true change happens when clinicians can deliver care that is evidence-based, replicable, and organized. By giving doctors the tools they need, we’re laying the groundwork for a day when precision brain health is not a niche option, but the expected standard.
Conclusion: Toward the First Reversal at Scale
Alzheimer’s has long been considered irreversible. That assumption is now being challenged.
The road to a new standard of care will require three things: robust placebo-controlled outcomes, integrated diagnostics, and organized care delivery. Add in insurance recognition, and we have the recipe for the first large-scale reversal of a chronic disease.
This won’t just change how we treat cognitive decline. It will change how we think about chronic disease altogether. If we can reverse Alzheimer’s, what else can we reverse?
That’s the future we’re building toward—one clinic, one patient, one community at a time.
Is this available in the U.K.? I am currently doing the ReCode training with Dr Bredesen, but organising tests and even getting U.K.
Drs engaged in undertaking cognitive assessments for patients with cognitive decline is a challenge.
"If we can reverse Alzheimer’s, what else can we reverse?" Thank you for thinking through this process and creating hope.